
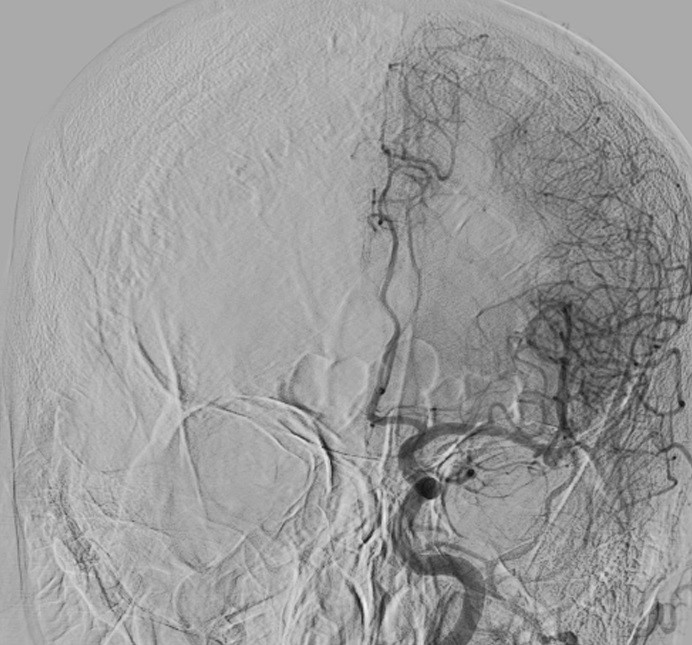
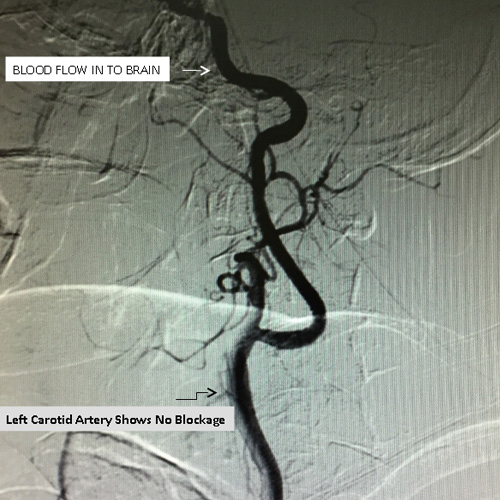
 62 year old male, diabetic, hypertensive, with history of temporary weakness of right arm and right leg. He was investigated and was found to have blockage in left neck vessel (Left Carotid Artery) by Doppler Ultrasound. He underwent Angiography of neck and brain vessel. Carotid Angioplasty was done to the disease segment.
62 year old male, diabetic, hypertensive, with history of temporary weakness of right arm and right leg. He was investigated and was found to have blockage in left neck vessel (Left Carotid Artery) by Doppler Ultrasound. He underwent Angiography of neck and brain vessel. Carotid Angioplasty was done to the disease segment.







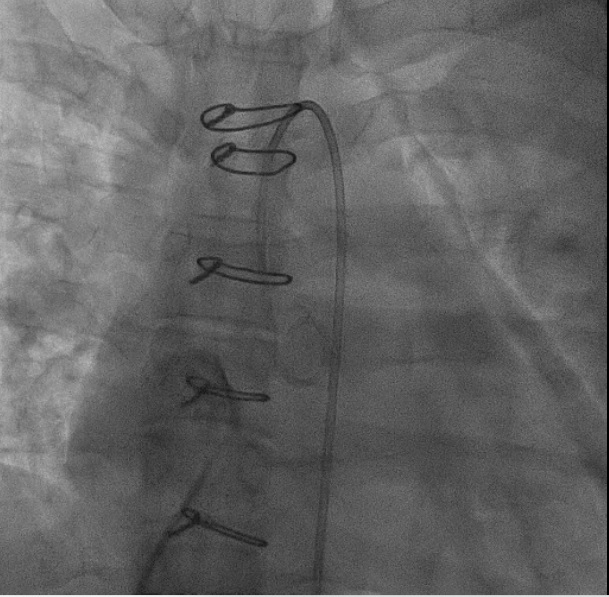
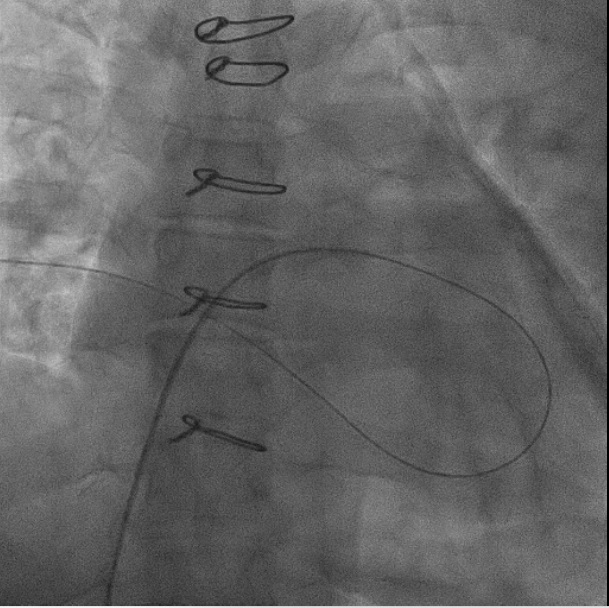
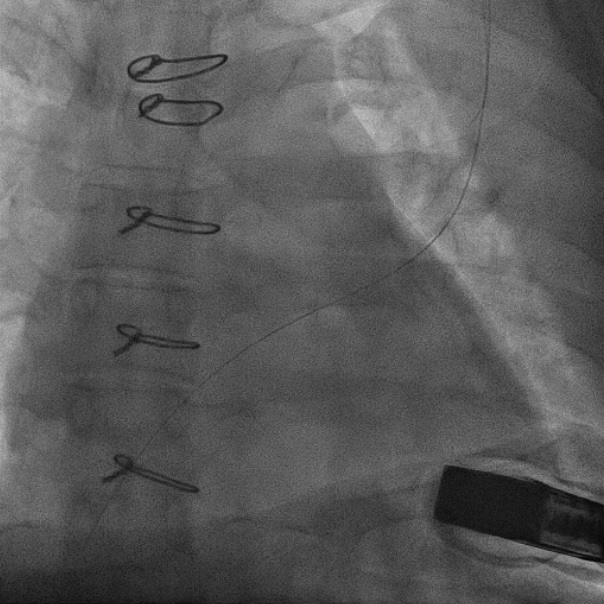
 42 yrs, active, office executive, gave up work for recurrent heart failure with frequent hospitalization. CRT-P device was implanted which improved her pumping action significantly.
42 yrs, active, office executive, gave up work for recurrent heart failure with frequent hospitalization. CRT-P device was implanted which improved her pumping action significantly.
Medication reduced no further hospitalization.
Back to active work and happy life.
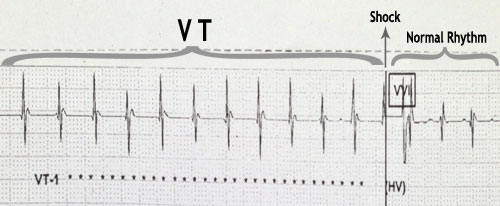
 46 years. 1st admission January 2013. Pulseless, unrecordable blood pressure, unconsciousness. CCU monitor – life threatning heart rhythm, which causes death(VT).
Rhythm restored in CCU by external electric shock. Life saved. Discharged on rhythm controlled medication with advice for urgent ICD implantation.
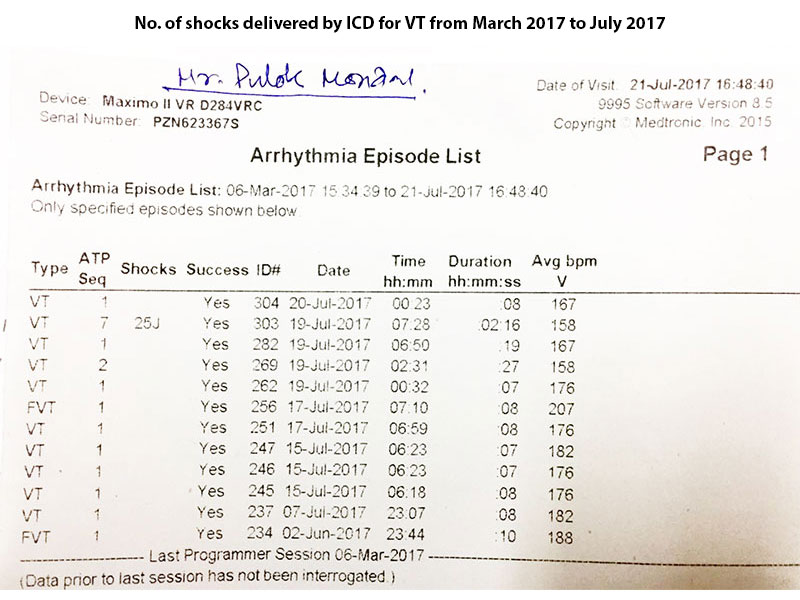
Readmitted 3rd August 2013, unconscious, no pulse, no BP, VT again shocked, saved. ICD implanted August 2013. Post discharge, at work, ICD activated by VT, shocked and patient saved outside hospital, not requiring further admission.
46 years. 1st admission January 2013. Pulseless, unrecordable blood pressure, unconsciousness. CCU monitor – life threatning heart rhythm, which causes death(VT).
Rhythm restored in CCU by external electric shock. Life saved. Discharged on rhythm controlled medication with advice for urgent ICD implantation.
Readmitted 3rd August 2013, unconscious, no pulse, no BP, VT again shocked, saved. ICD implanted August 2013. Post discharge, at work, ICD activated by VT, shocked and patient saved outside hospital, not requiring further admission. 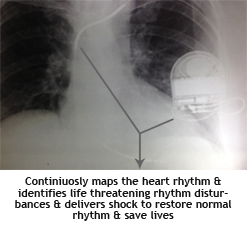
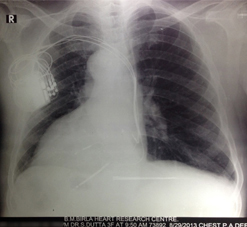
 When the heart is displaced since birth to the opposite side (dextrocardio) CRT-D (CRT-P + ICD) implantation becomes a complex procedure.
This 57 years old gentleman with heart displaced to the right side as seen in this X-Ray was implanted with CRT-D device to prevent recurrent admission with heart failure. He was in end stage heart failure on maximal medication with past history of recurrent heart failure.
When the heart is displaced since birth to the opposite side (dextrocardio) CRT-D (CRT-P + ICD) implantation becomes a complex procedure.
This 57 years old gentleman with heart displaced to the right side as seen in this X-Ray was implanted with CRT-D device to prevent recurrent admission with heart failure. He was in end stage heart failure on maximal medication with past history of recurrent heart failure.
After CRT-D goes home walking and is well with no further heart failure. He was admitted recently once with shock delivered by ICD device converting life threatening rhythm (VT) to normal rhythm at home. Discharged same day.
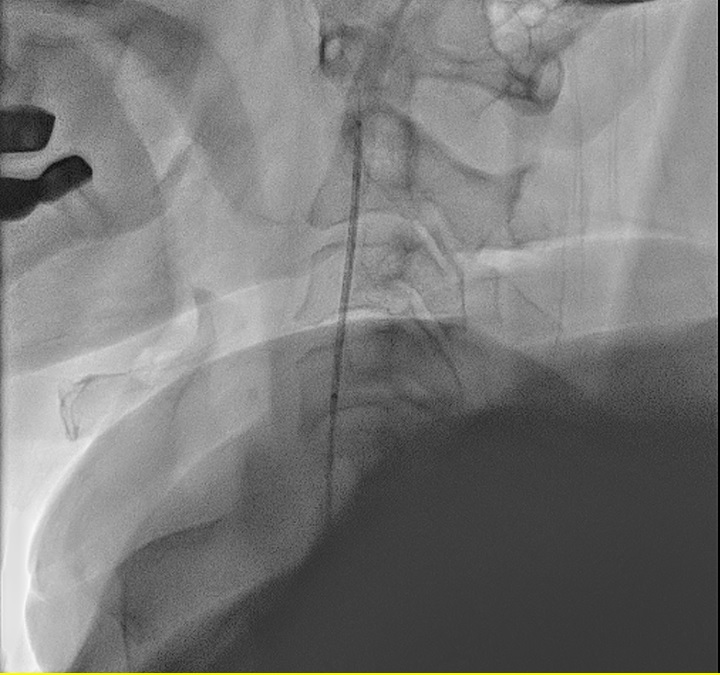
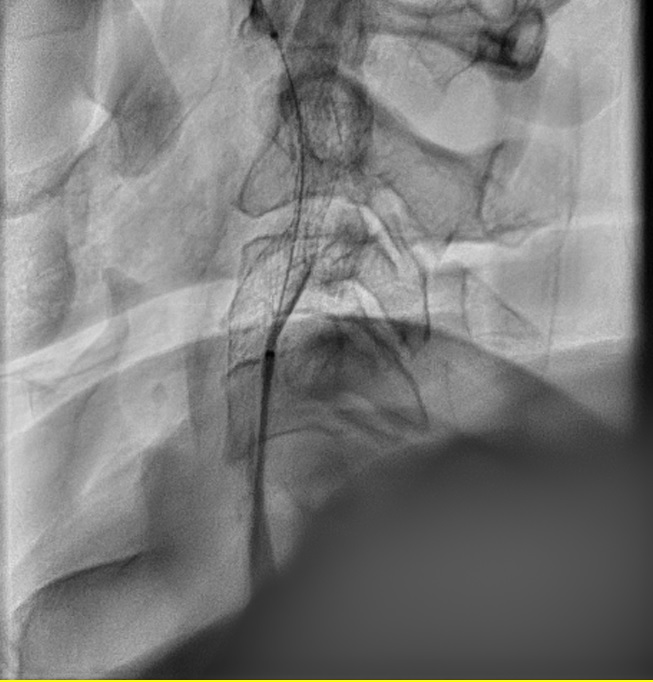
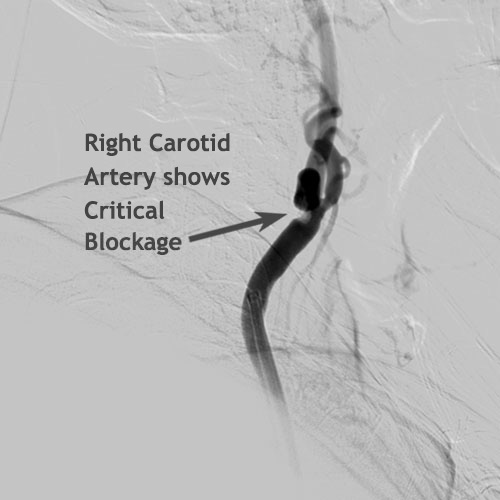
 55 year old woman with temporary weakness of left arm and leg with immediate recovery was found to have blockage in right neck vessel (Right Carotid Artery). Small fat particle had temporarily dislodged into her brain circulation leading to the above symptoms. Larger particles usually lead to brain stroke.
55 year old woman with temporary weakness of left arm and leg with immediate recovery was found to have blockage in right neck vessel (Right Carotid Artery). Small fat particle had temporarily dislodged into her brain circulation leading to the above symptoms. Larger particles usually lead to brain stroke.
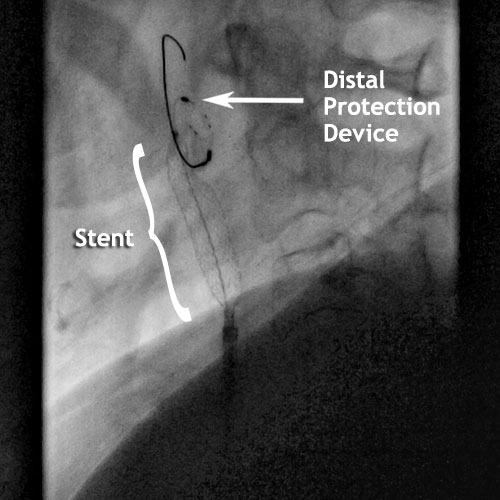
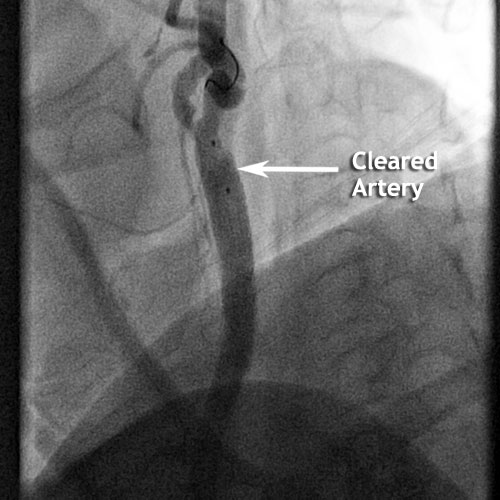
She underwent treatment by Stenting of Right Carotid Artery (Carotid Angioplasty) on 06.07.2012 with Distal Protection Device. Distal Protection Device prevents clots from entering into brain circulation during stenting causing brain stroke during stenting procedure.
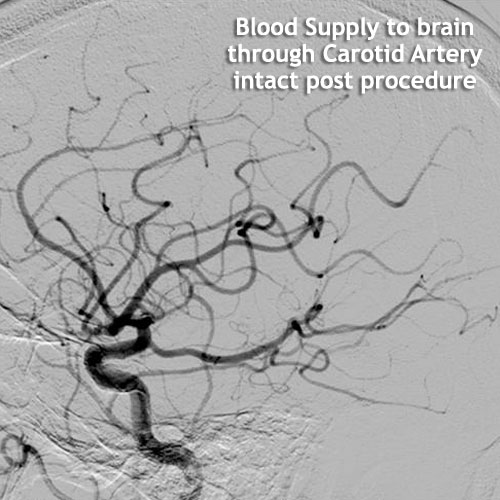
She’s doing well till date with no subsequent recurrence of symptoms and no brain stroke.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
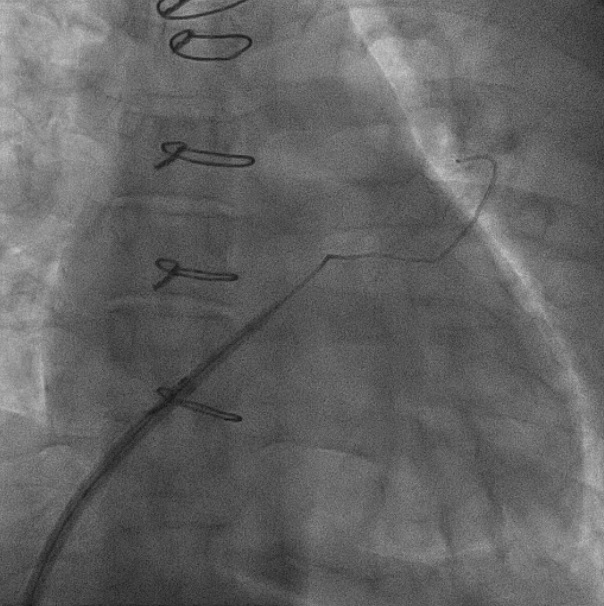
 46 years old gentleman was referred for Bypass Surgery because of main three heart artery blockage.
46 years old gentleman was referred for Bypass Surgery because of main three heart artery blockage.
FFR study done on 08.04.2013. It confirmed that only single artery blockage was critical. Hence single vessel stenting was done in same sitting. Patient well.
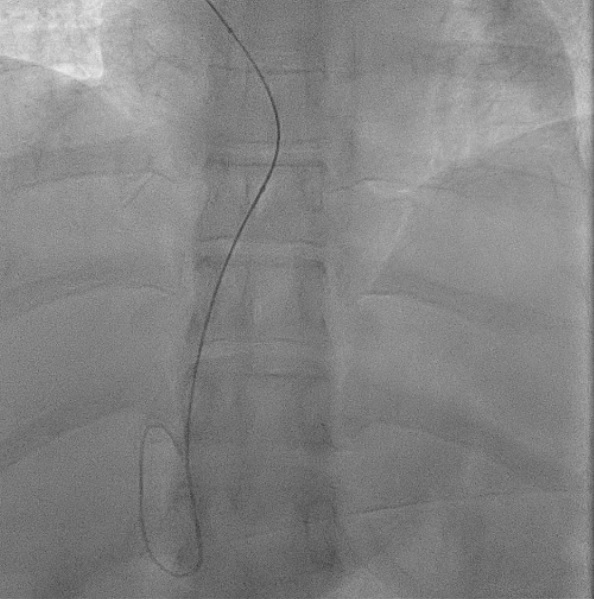
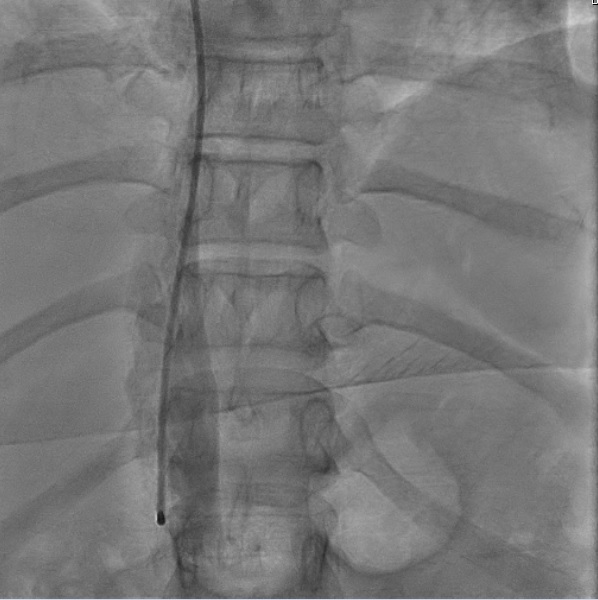
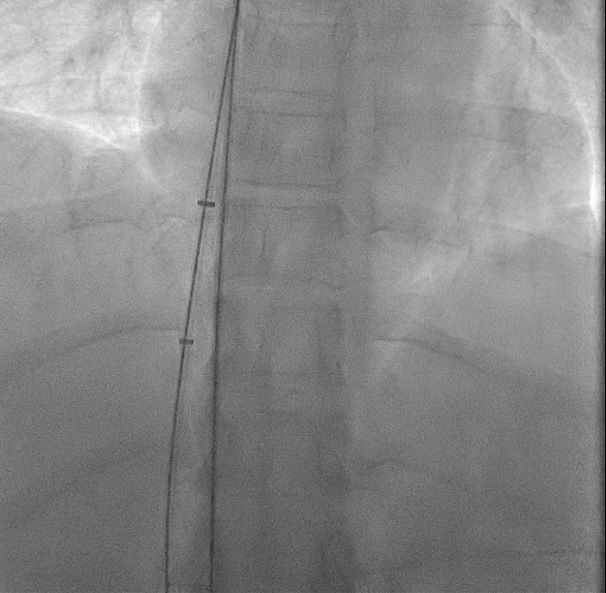
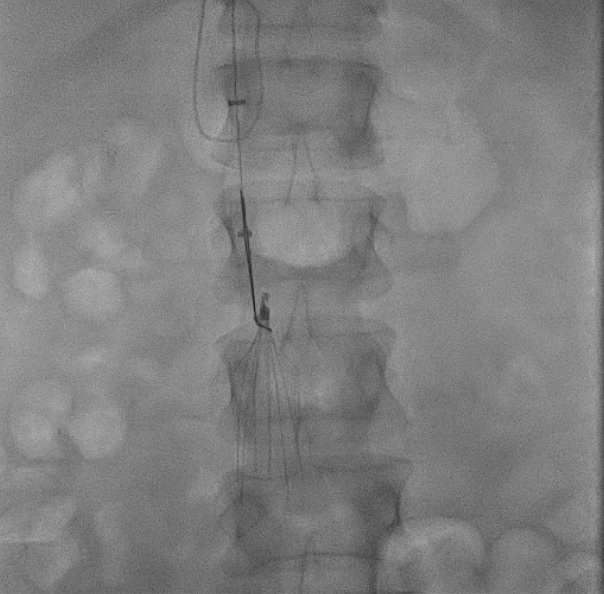
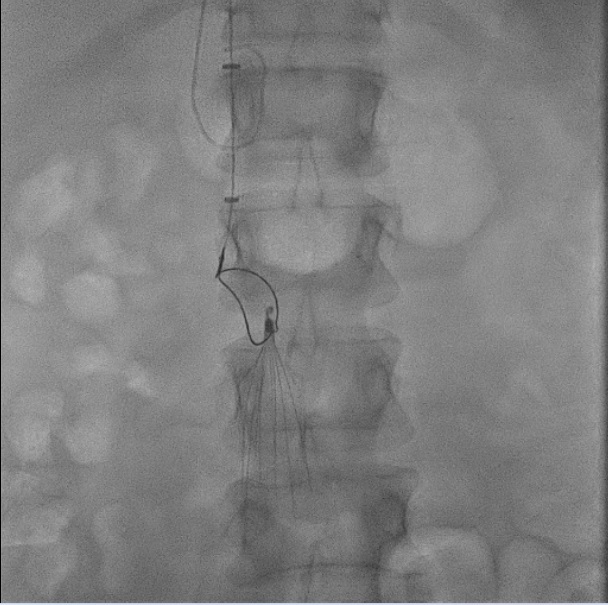
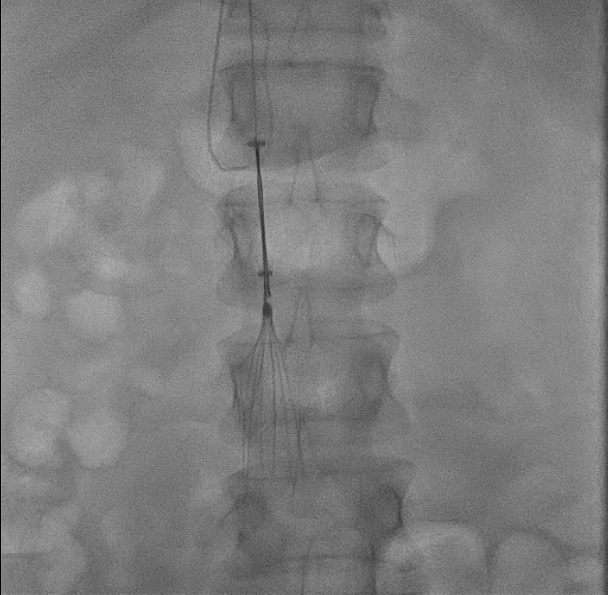
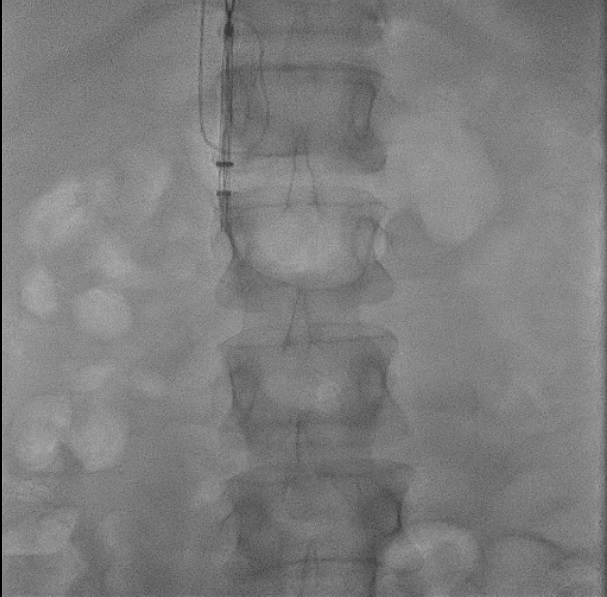
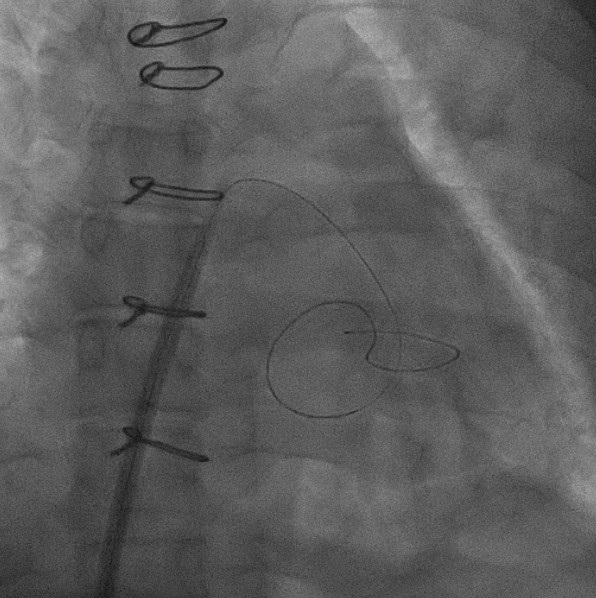
 56 yr old male was admitted with painful, unprovoked, severe swelling of left leg.
Dopler ultrasound confirmed clotting in left leg veins.
56 yr old male was admitted with painful, unprovoked, severe swelling of left leg.
Dopler ultrasound confirmed clotting in left leg veins.
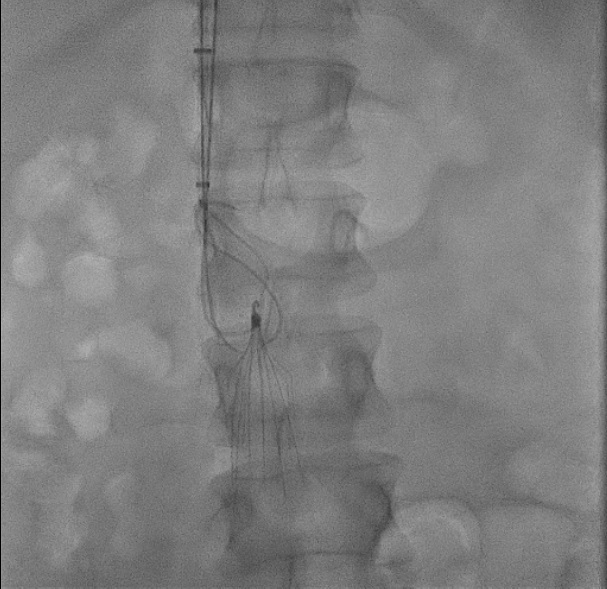
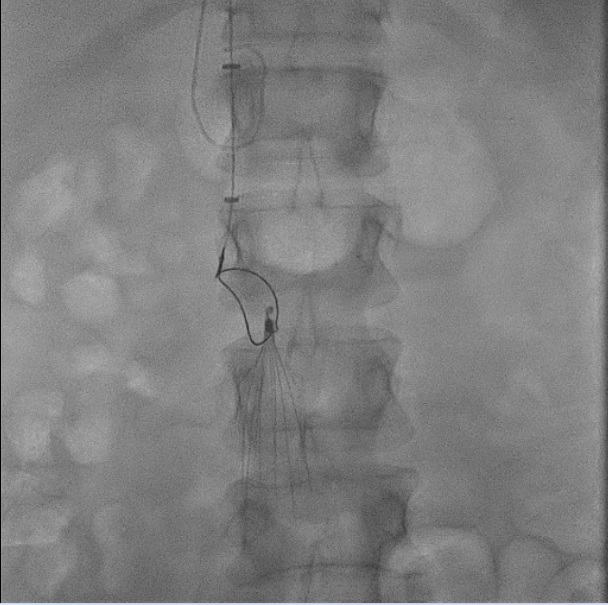
Complication: Clot dislodgement from leg to lungs causing pulmonary embolism and sudden death.
Treatment: Clot buster injection was administered to dissolve clots in leg and IVC Filter was placed above leg veins (IVC) to trap particles dislodged during dissolving clots and prevent lung complication (Pulmonary Embolism) leading to sudden death during treatment.

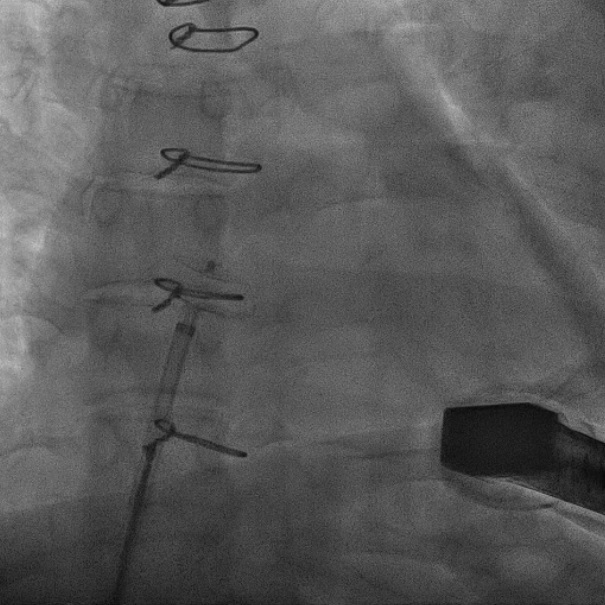
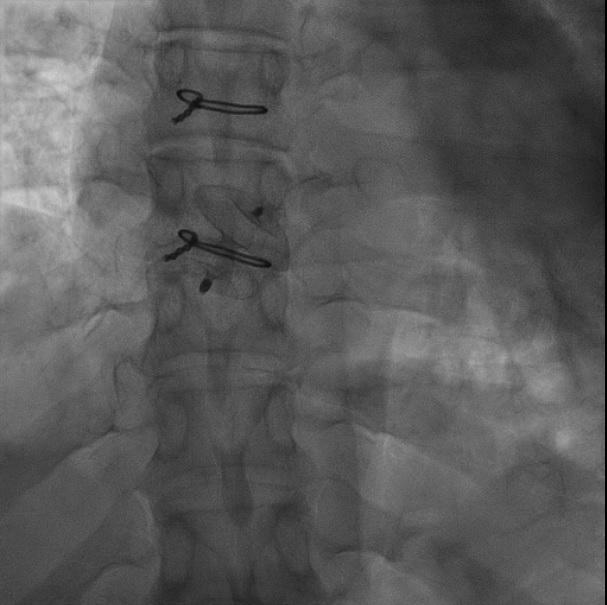
 68 year old male with increasing abdominal and lower back pain. Gastroenterologist and Orthopaedic consultation were normal.
68 year old male with increasing abdominal and lower back pain. Gastroenterologist and Orthopaedic consultation were normal.
Diagnosis: Large abdominal aortic aneurysm diagonised by abdominal ultrasound. Above symptoms were suggestive of impending rupture of sac causing death.
Treatment: Stenting done with a self expanding stent covered by Teflon. This stent comes compressed and is passed from leg and released below kidney arteries within the sac from healthy segment of blood vessel above the sac to below the sac. Blood then flows through tube (covered Stent) preventing blood leaking into surrounding sac. The blood trapped in the sac clots and the sac shrinks and aneurysm disappears. Final results in video 4 confirms blood flowing from normal section of abdominal aorta flows through stent (covered tube) to both legs with no leakage into aneurysm sac.
 78 year old male was admitted with shortness of breath, fainting and fatigue. Past history of bypass surgery 18 years back. Check angiogram confirmed bypass grafts to be OK.
78 year old male was admitted with shortness of breath, fainting and fatigue. Past history of bypass surgery 18 years back. Check angiogram confirmed bypass grafts to be OK.
Diagnosis: New problem — Aortic valve the main door which allows blood from heart to pump to our body was blocked and now required valve replacement with open heart operation. Surgical team felt, TAVR device to be implanted (Non-surgical valve replacement) as risk of open heart surgery was high after bypass surgery and advanced age.
Treatment: TAVR done successfully from leg and patient discharged on January 2021 after 3 days. Last follow up January 2022 doing well..
Pictures and videos below gives us an idea about the implantation.
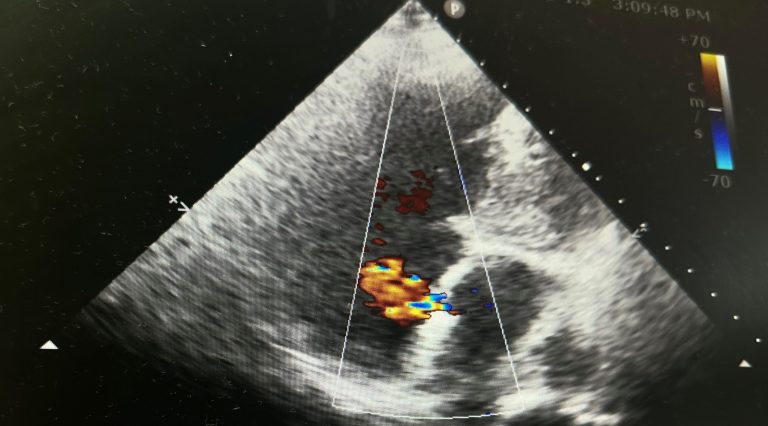
 54 year old lady was diagnosed to have hole in her heart by Echo-cardiogram in Bangladesh, and was advised Device Closure.
54 year old lady was diagnosed to have hole in her heart by Echo-cardiogram in Bangladesh, and was advised Device Closure.
She presented with shortness of breath on effort.
Pictures and videos below gives us an idea about the procedure.
 56 year lady who had surgical closure with post surgical patch closure of ASD which developed leakage.
56 year lady who had surgical closure with post surgical patch closure of ASD which developed leakage.
Diagnosis: This leakage has been confirmed by echo. Risk of reoperation was high.
Treatment: The reoperation was avoided and device closure of the patient was done successfully.
 48 year old gentleman with shortness of breath was admitted.
48 year old gentleman with shortness of breath was admitted.
Diagnosis: He had routine echo cardiogram by his physician which incidentally diagnosed PDA with left to right shunt with elevated pressure due to shunt causing his symptoms.
Treatment: Above mentioned procedure was conducted to him and he was relieved of his symptoms.
78 year old diabetic, hypertensive patient had severe symptoms of angina in spite of maximum medication.
Diagnosis: Coronary angiography showed severe calcified blockage.
Intravascular imaging was done which showed patient would require rotablation to debunk calcium before stenting.
Treatment: Rotablation was done to debunk calcium.
Pre and post imaging showed adequate lumen after stenting.
+91 98305 06845
Mobile (Secretary)
shuvodutta@yahoo.com
Doctor's Email


